Preserving Prosperity By Extending Health Span Of Society One Patient At A Time


Nee Soon Clinic
29 May 2026
How cardiovascular risk determines your personal LDL goal — and what to do when standard treatment isn't enough
When a blood test comes back showing high LDL cholesterol, one of the first questions patients ask is: what number should I be aiming for? It is a reasonable question — and the answer is more nuanced than most people expect.
There is no single universal LDL target that applies to everyone. The number your doctor is aiming for depends on your overall cardiovascular risk profile. A 35-year-old with no other risk factors and a mildly elevated LDL has a very different target from a 60-year-old who has already had a heart attack.
Treating both to the same LDL level would either over-treat the younger patient or dangerously under-treat the older one.
Understanding your personal LDL target — and where it comes from — is one of the most practical things you can do to take ownership of your cardiovascular health.
Why LDL Targets Are Not One-Size-Fits-All
LDL cholesterol does not cause harm in isolation. It causes harm in the context of the cardiovascular system as a whole — interacting with blood pressure, blood sugar, smoking status, age, sex, kidney function, family history, and whether existing cardiovascular disease or damage is already present.
The scientific framework used to set LDL targets reflects this. Rather than applying a population-wide threshold, international guidelines — including those of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS), which inform clinical practice in Singapore — stratify patients into cardiovascular risk categories. Each category carries a different recommended LDL target.
The logic is straightforward: the higher your overall risk, the more aggressively LDL needs to be lowered to meaningfully reduce that risk.
The Four Cardiovascular Risk Categories
Risk Category | 10-Year Cardiovascular Risk | Typical Patient Profile |
Very High | ≥10% or established disease | Previous heart attack or stroke; FH with cardiovascular disease; severe chronic kidney disease; high-risk diabetes with organ damage |
High | 5–10% | Familial hypercholesterolaemia (FH) without cardiovascular disease; most people with type 2 diabetes; moderately reduced kidney function; single markedly elevated risk factor |
Moderate | 1–5% | Multiple risk factors present but no single dominant one; 10-year estimated risk between 1 and 5% |
Low | <1% | Young patients with few or no risk factors; no family history of premature cardiovascular disease |
Risk estimation for patients without established cardiovascular disease is typically calculated using a validated tool. In European-aligned guidelines, the SCORE (Systematic COronary Risk Estimation) model is used. Your doctor calculates this based on your age, sex, smoking status, blood pressure, and total cholesterol.
LDL Cholesterol Targets by Risk Level
Once your risk category is established, your LDL target follows:
Risk Category | LDL Target | Additional Requirement |
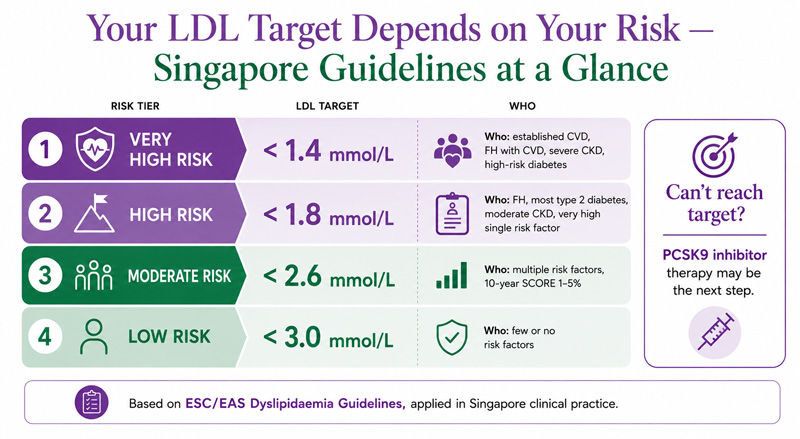
Very High Risk | <1.4 mmol/L | AND a reduction of ≥50% from your untreated baseline LDL |
High Risk | <1.8 mmol/L | AND a reduction of ≥50% from your untreated baseline LDL |
Moderate Risk | <2.6 mmol/L | — |
Low Risk | <3.0 mmol/L | — |
Two points are worth highlighting here.
First, for very high and high-risk patients, the target is not just a number — it is a number and a proportional reduction. A patient with a baseline LDL of 5.0 mmol/L who achieves 2.0 mmol/L has technically met the <1.8 target for high-risk patients, but has not yet achieved the required ≥50% reduction. Both criteria need to be met.
Second, these targets may be revised downward in future guideline iterations as accumulating trial evidence shows benefit from even lower LDL levels in very high-risk populations. If you are being managed under updated guidelines, your doctor will apply the most current thresholds.
How Your Risk Category Is Determined
Your doctor will consider the following in assigning your risk category:
Established cardiovascular disease places you automatically in the very high-risk category. This includes a documented history of heart attack, angina, stroke or TIA, coronary revascularisation, or peripheral artery disease.
Diabetes typically places patients in the high-risk category at minimum. Those with type 2 diabetes who also have evidence of target organ damage — diabetic kidney disease, retinopathy, or significant neuropathy — or who have had the condition for more than 10 years alongside other risk factors may be classified as very high risk.
Chronic kidney disease (CKD) at moderate severity (eGFR 30–59 mL/min/1.73m²) is classified as high risk; severe CKD (eGFR below 30) is classified as very high risk.
Familial hypercholesterolaemia (FH) places patients in the high-risk category by default. The presence of cardiovascular disease in an FH patient upgrades them to very high risk. For a detailed explanation of FH, read our guide to familial hypercholesterolaemia in Singapore →.
Single markedly elevated risk factors — such as LDL above 4.9 mmol/L or blood pressure of 180/110 mmHg or higher — can independently qualify a patient for the high-risk category even in the absence of other factors.
Estimated 10-year cardiovascular risk using SCORE or a similar validated tool determines categorisation for patients who do not fall into any of the above established groups.
What If You Cannot Reach Your LDL Target?
For many patients — particularly those in the high and very high-risk categories with significantly elevated baseline LDL — reaching the target on standard therapy alone is genuinely difficult.
Maximum-intensity statin therapy (the highest dose of the most potent statin tolerated) is the foundation of treatment and can reduce LDL by 40 to 55%.
Adding ezetimibe on top of statin therapy provides an additional 15 to 25% LDL reduction by blocking intestinal cholesterol absorption.
For patients who remain above target after optimising both, or for those who cannot tolerate adequate statin doses, PCSK9 inhibitor therapy is the most effective additional treatment available. PCSK9 inhibitors reduce LDL by 50 to 60% on top of existing therapy — a magnitude of reduction that can bring even very high-risk patients with persistently elevated LDL into target range.
For a full explanation of PCSK9 inhibitor therapy — how it works, who qualifies, and what the treatment involves in Singapore — read our dedicated guide to PCSK9 inhibitors in Singapore →.
Beyond LDL: Other Lipid Markers Your Doctor Watches
LDL is the primary target, but it is not the only lipid marker your doctor will monitor.
Non-HDL cholesterol captures all atherogenic (plaque-forming) lipoproteins in a single figure — LDL plus VLDL and IDL. It is calculated simply as total cholesterol minus HDL. Non-HDL targets are 0.8 mmol/L higher than the corresponding LDL targets (so <2.2 mmol/L for very high-risk patients).
Triglycerides above 1.7 mmol/L suggest suboptimal metabolic health and may indicate higher cardiovascular risk independent of LDL. Severely elevated triglycerides (above 10 mmol/L) carry a risk of acute pancreatitis and require specific treatment.
HDL cholesterol (the "good" cholesterol) below 1.0 mmol/L in men and below 1.2 mmol/L in women is associated with higher cardiovascular risk. There are currently no approved medications with a primary indication of raising HDL, but low HDL is factored into overall risk assessment.
Lipoprotein(a) [Lp(a)] is an LDL-like particle whose levels are genetically determined and largely unresponsive to statin therapy. Elevated Lp(a) is an independent cardiovascular risk factor. It is worth measuring at least once in your lifetime, particularly if you have a family history of premature cardiovascular disease.
How Often Should LDL Be Checked?
The frequency of monitoring depends on your treatment phase and risk level:
Before starting treatment: A fasting lipid panel establishes your baseline LDL, which is needed to calculate the percentage reduction target for high and very high-risk patients.
After starting or changing therapy: Recheck at 8 to 12 weeks to assess the treatment response.
Once stable on treatment: Annual monitoring is standard for most patients on long-term therapy, or sooner if risk factors change.
If symptoms arise: Any new cardiovascular symptoms, or concerns about medication side effects, should prompt an earlier review.
Your doctor may also check liver function and, for patients on statins, creatine kinase (CK) at the initiation of therapy or if muscle symptoms develop.
Frequently Asked Questions
My LDL is 2.0 mmol/L. Is that good enough?
It depends entirely on your risk category. For a moderate-risk patient, 2.0 mmol/L is well within target. For a very high-risk patient — for example, someone who has had a previous heart attack — the target is below 1.4 mmol/L, and 2.0 mmol/L would indicate that treatment needs to be intensified.
My doctor says my LDL is normal, but I've read that lower is always better. Who is right?
Both statements have truth in them. For lower-risk individuals, there is no clinically meaningful benefit to driving LDL extremely low, and unnecessarily aggressive treatment carries side effect risk. For high and very high-risk patients, evidence from landmark cardiovascular trials does support the principle that lower LDL reduces events further — which is why the guideline targets for these groups are now considerably below what was recommended a decade ago.
Can I achieve my LDL target through diet alone?
For low and moderate-risk patients with mildly elevated LDL, lifestyle changes — reducing saturated fat, increasing soluble fibre, losing weight, and exercising regularly — can meaningfully lower LDL, sometimes enough to reach target. For high and very high-risk patients, or anyone with significantly elevated baseline LDL, medication is almost always required in addition to lifestyle management.
What is a "baseline LDL" and why does it matter?
Your baseline LDL is the level measured before treatment begins. For high and very high-risk patients, guidelines require not only achieving an absolute LDL target but also achieving at least a 50% reduction from this baseline. If your pre-treatment LDL was 4.0 mmol/L, a 50% reduction would bring you to 2.0 mmol/L — and in the high-risk category, that would also satisfy the <1.8 mmol/L threshold.
How do I find out what risk category I am in?
Ask your doctor directly. They will assess your cardiovascular history, diabetes and kidney status, blood pressure, smoking history, and blood lipid results to calculate your risk. If you have concerns about your LDL or cardiovascular risk, our high cholesterol service page explains how Nee Soon Clinic approaches this assessment.
Final Thoughts
Your LDL target is not a number picked at random — it reflects a careful weighing of your individual cardiovascular risk and the evidence on how much LDL reduction is needed to make a meaningful difference for someone in your position. Understanding your risk category, knowing your current LDL, and asking your doctor whether you have reached your personal target are three practical steps that put you in control of the conversation.
If standard treatments are not getting you to your target — whether because of side effects, insufficient response, or a very high starting LDL — it is worth asking specifically about what additional options, including PCSK9 inhibitor therapy, might be appropriate for your situation.
Disclaimer: The information provided in this article is for informational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. The content is not intended to be a comprehensive source of information and should not be relied upon as such. Reliance on any information provided in this article is solely at your own risk. The authors and the publisher do not endorse or recommend any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned in the article. Any reliance on the information in this article is solely at the reader's own risk.
Official info: https://www.repatha.com/ and https://www.leqvio.com/
779 Yishun Ave 2, #01-1547, Singapore 760779
Tel: 6721 9796
